
Introduction
Mental health billing has always been complex. For psychiatrists, behavioral health providers, and practice managers, claim denials, changing payer rules, and documentation requirements create ongoing revenue challenges. According to Experian Health’s 2025 State of Claims Report, 41% of US healthcare providers now report that more than one in ten of their claims get denied and that number has climbed steadily every year since 2022.
Mental health billing guidelines in 2026 are the payer and federal rules that govern how behavioral health services are coded, documented, and reimbursed. They include CPT coding rules, telehealth billing requirements, prior authorization policies, and compliance standards under the Mental Health Parity and Addiction Equity Act (MHPAEA). Behavioral health utilization has jumped 62.6% from 2018 to 2024, according to Trilliant Health’s 2025 report and demand is still growing.
In this guide, you’ll find everything you need to bill correctly, stay compliant, and protect your revenue.
Key Updates in Mental Health Billing for 2026
Why Is Mental Health Billing So Complex in 2026?
Mental health billing is complex because each payer applies different rules on top of federal guidelines, especially for telehealth, authorization, and documentation requirements.
Here’s what physicians and billing managers need to know:
1. Telehealth Flexibilities Extended Medicare has extended many telehealth provisions that originated during the COVID-19 public health emergency. Audio-only mental health visits remain reimbursable for patients who lack video capability, though specific documentation requirements apply.
2. Collaborative Care Model (CoCM) Expansion Payers are increasingly reimbursing for integrated behavioral health under the Collaborative Care Model (CPT codes 99492, 99493, 99494). If your practice hasn’t evaluated CoCM billing, you may be leaving revenue on the table.
3. Stricter Medical Necessity Documentation Both Medicare and commercial payers have heightened scrutiny on medical necessity for ongoing psychotherapy. Session notes must clearly justify continued treatment, not just describe what occurred during the visit.
4. Prior Authorization Requirements Tightening Many commercial payers now require authorization for more than 6–8 sessions upfront. Failure to obtain timely authorization is one of the leading causes of claim denial in mental health billing. Source AMA
5. Modifier Compliance Under Audit CMS and commercial payers are actively auditing modifier use, particularly GT, 95, and POS codes for telehealth. Incorrect modifier application results in denials, recoupments, and compliance risk.
6. Telehealth Denials Are Spiking According to MDaudit’s 2025 benchmarking data, telehealth-related claim denials rose 84% from 2024 to 2025. The most common culprit? Incorrect modifier or Place of Service code. These are entirely preventable errors; and they’re costing behavioral health practices real money.
7. Behavioral health provider eligibility continues expanding, including changes affecting Licensed Mental Health Counselors (LMHCs) and Licensed Marriage and Family Therapists (LMFTs), where applicable.
Important Compliance Note:
Providers should not assume CPT 99492–99494 have been universally replaced. Many commercial payers and some Medicaid programs continue to use CPT-based CoCM billing. However, Medicare Advantage and APCM-linked structures may require HCPCS-based reporting depending on plan guidance.
Before billing CoCM services in 2026, practices should:
- Verify payer-specific CoCM billing requirements
- Confirm whether CPT or HCPCS structure applies
- Align documentation with time-based CoCM requirements
- Ensure correct integration with APCM or care management programs
Why Do Mental Health Claims Get Denied
Using the correct CPT codes for psychotherapy is non-negotiable. Here’s a practical reference:
Psychotherapy CPT Codes
| CPT Code | Description | Time |
|---|---|---|
| 90832 | Psychotherapy, office | 30 min |
| 90834 | Psychotherapy, office | 45 min |
| 90837 | Psychotherapy, office | 60 min |
| 90839 | Psychotherapy for crisis, first 60 min | 60 min |
| 90840 | Crisis psychotherapy, each additional 30 min | 30 min |
| 90847 | Family psychotherapy with patient present | — |
| 90853 | Group psychotherapy | — |
Psychiatric Evaluation & Management
| CPT Code | Description |
|---|---|
| 90791 | Psychiatric diagnostic evaluation |
| 90792 | Psychiatric diagnostic evaluation with medical services |
| 99213–99215 | E/M visits (medication management, office) |
Add-On Codes (Psychotherapy with E/M)
When medication management and psychotherapy occur in the same visit, use the psychotherapy add-on codes alongside E/M codes:
- 90833 — 30 min psychotherapy with E/M
- 90836 — 45 min psychotherapy with E/M
- 90838 — 60 min psychotherapy with E/M
Collaborative Care Model
| CPT Code | Description |
|---|---|
| 99492 | Initial month, 70+ min |
| 99493 | Subsequent month, 60+ min |
| 99494 | Additional 30 min (add-on) |
Billing the wrong code or skipping add-on codes directly reduces your reimbursement. Audit your coding patterns quarterly.
Medicare Reimbursement Considerations for Mental Health Billing in 2026
Correct CPT coding is only one part of successful mental health billing. Reimbursement also depends on factors such as Medicare payment policies, Relative Value Units (RVUs), geographic adjustments, provider participation status, and payer contracts.
For Medicare services, reimbursement amounts may vary based on:
- Geographic locality
- Provider enrollment status
- Medicare participation status
- Applicable payment adjustments
- Annual Physician Fee Schedule updates
Practices should review current CMS Physician Fee Schedule updates and payer-specific contracts to confirm reimbursement expectations for 2026.
How Do You Bill Telehealth for Mental Health in 2026?
Telehealth has fundamentally changed how behavioral health care is delivered. In 2024, nearly 66% of all behavioral health visits were delivered via telehealth. That shift has made getting telehealth billing right one of the most important skills in behavioral health revenue cycle management.
Telehealth billing for mental health remains one of the highest-risk areas for denials. Here’s how to bill it correctly in 2026:
Place of Service (POS) Codes
- POS 02 — Telehealth provided other than in patient’s home
- POS 10 — Telehealth provided in patient’s home
Required Modifiers
Telehealth Modifiers for Mental Health Billing
Modifier 95
Modifier 95 is commonly used for synchronous interactive audio-video telemedicine services when required by commercial payers and certain Medicare Advantage plans. Source AAPC
Modifier 93
Modifier 93 may be used for synchronous audio-only telemedicine services when permitted by the payer.
Modifier GT
Modifier GT is not generally required for Medicare Part B professional claims. Medicare professional claims typically use appropriate Place of Service codes, such as POS 02 or POS 10, based on CMS requirements. (CMS)
Modifier GT may still apply in specific institutional billing situations, including certain Critical Access Hospital (CAH) Method II claims.
Providers should always confirm payer-specific modifier requirements before claim submission.
For Example: The CPT code itself doesn’t change for telehealth. A 38-52 min individual psychotherapy session is still billed as 90834 whether it happens in your office or over a video call. The modifier and POS code are what tells the payer it was delivered remotely.
Audio-Only Billing Medicare permits audio-only billing for mental health services when the patient is unable to use video technology and documents this limitation. The provider must note the audio-only nature and clinical justification in the record.
Key Rule: The CPT code for telehealth billing mental health services stays the same as in-person; the modifier and POS code are what distinguish the claim. Billing with the wrong combination is the most common telehealth denial trigger.
State-Specific Rules Commercial payers often follow state telehealth parity laws. Confirm with each payer whether synchronous audio-only is covered before billing some still require video for full reimbursement.
Documentation Requirements for Compliance & Reimbursement
Poor documentation is the silent revenue killer. Auditors and payers look for specific elements that many providers overlook.
Every session note must include:
- Date and duration of service
- Clinical presentation
- Interventions performed
- Treatment response
- Medical necessity justification
- Risk assessment (if applicable)
- Treatment plan updates
For psychiatric E/M visits, documentation must also support the level of medical decision-making (MDM) or time-based billing consistent with the selected E/M code.
Audit-Ready Tip: If your note could apply to any patient on any day, it will not survive a payer audit. Documentation must be specific, individualized, and clinically defensible.
Why Do Mental Health Claims Get Denied?
According to the MGMA’s 2024 Benchmarking Report on Denials and Appeals, more than half of US healthcare organizations now report denial rates exceeding 10%. In behavioral health, where coding complexity and payer-specific rules overlap, the reasons are often preventable.
Common causes of mental health claim denials include:
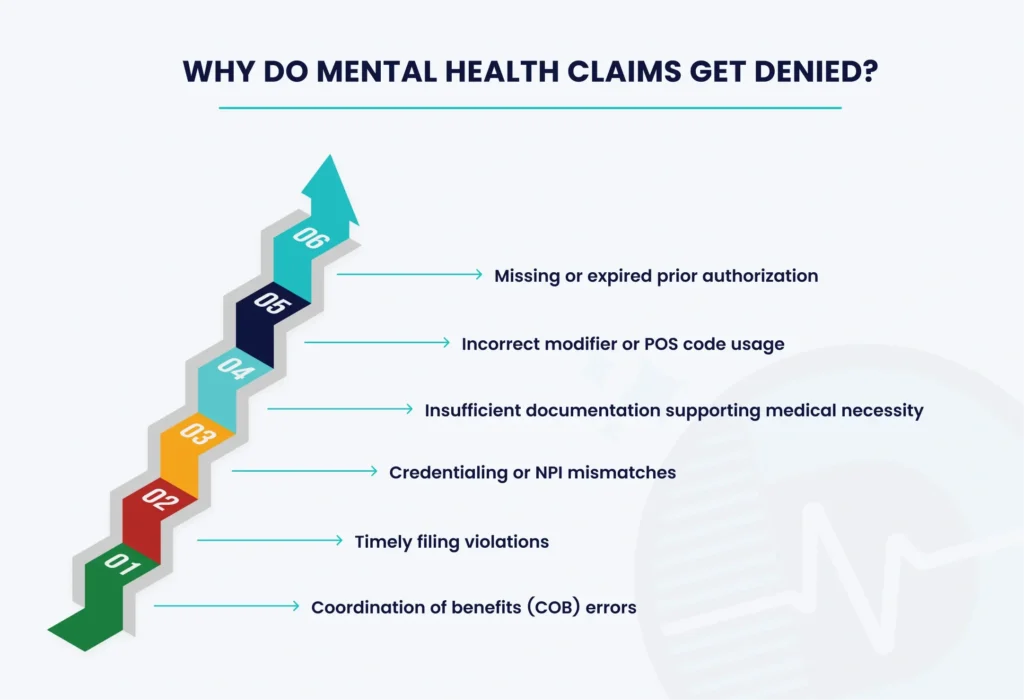
If the same denial reason appears repeatedly each month, it may indicate a workflow issue rather than an isolated claim error.
Authorization Management: A Major Denial Prevention Strategy
Authorization failures are one of the most common and preventable causes of mental health claim denials. A proactive authorization workflow helps practices avoid unpaid services and unnecessary appeals.
Pre-Visit Verification
Before appointments, confirm:
- Active behavioral health benefits (not just general coverage)
- Payer-specific session limits and authorization requirements
- Provider credentialing status with the payer
- Telehealth coverage eligibility
- Behavioral health carve-outs managed by third-party administrators
Authorization Tracking Process
Maintain a system to:
- Track authorization start and expiration dates
- Request renewals 10–14 days before expiration
- Attach authorization numbers to claim submissions
- Maintain records of payer communications and approval details
Preventing authorization issues before claim submission is more effective than appealing denials after services have already been provided.
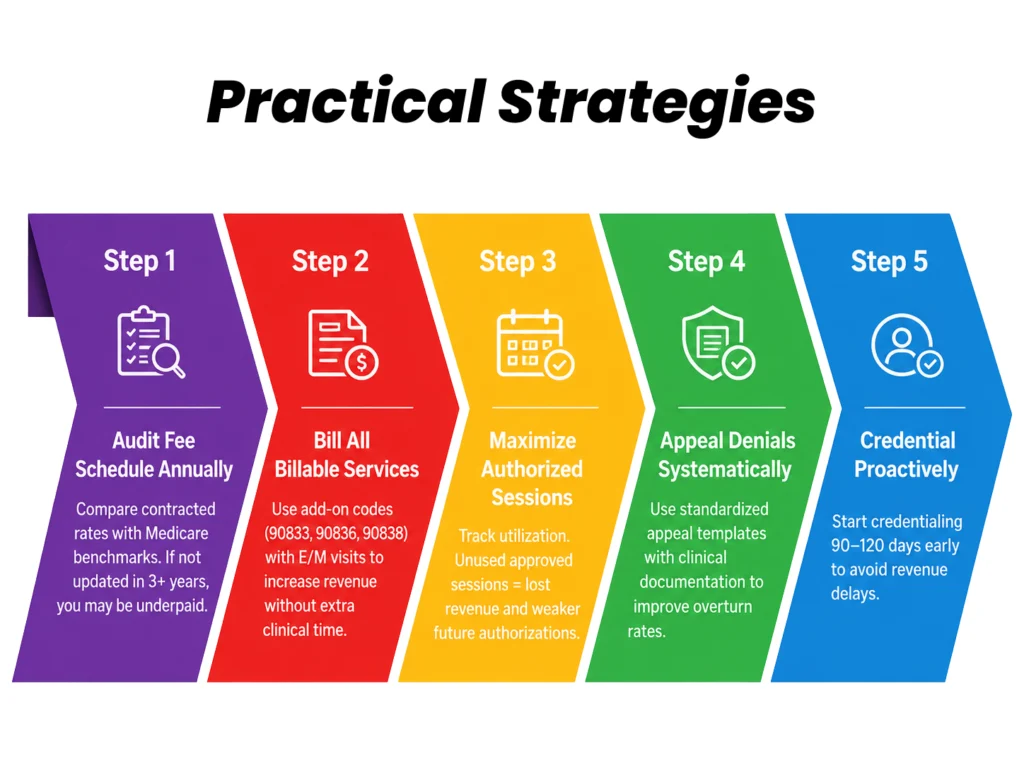
How to Improve Mental Health Billing Reimbursement
Improving reimbursement starts upstream in your billing process:
Compliance Review Checklist
Use this checklist to assess your practice’s current compliance posture
- CPT codes updated for 2026
- Telehealth modifiers correctly applied
- Documentation meets medical necessity standards
- Prior authorization tracking in place
- Denials reviewed monthly
- HIPAA compliance maintained
- Credentialing records accurate
- Fee schedules benchmarked annually
This checklist works as a starting point. Larger practices may need a more formal compliance program with a designated compliance officer.
Outsourcing Mental Health Billing Services
Managing mental health billing in-house is increasingly difficult. Payer policies change frequently, telehealth rules vary by state and payer, and credentialing alone can consume significant staff bandwidth.
Many behavioral health practices; from solo psychiatrists to multi-provider clinics are turning to specialized medical billing services who focus exclusively on behavioral health rcm.
What to Look for in a Billing Partner:
A qualified mental health billing partner should provide:
- Experience with behavioral health billing guidelines and psychiatric CPT codes
- Active denial management and appeals support
- Transparent reporting on collections, denials, and A/R performance
- HIPAA-compliant technology and data security
- Credentialing support when needed
The right partner helps identify coding issues, prevent authorization gaps, and recover revenue lost to denials and underpayments.
FAQs
Q1: What CPT code is used for a 45-minute individual psychotherapy session?
Use CPT 90834 for a 45-minute individual psychotherapy session. If psychotherapy and medication management are provided during the same visit, report CPT 90836 with the appropriate E/M code when documentation supports both services.
Q2: How many psychotherapy sessions does Medicare cover?
Medicare does not set a fixed session limit for medically necessary psychotherapy. Coverage depends on whether documentation supports the ongoing clinical need for treatment.
Q3: What is the timely filing limit for mental health claims?
Timely filing limits vary by payer. Medicare generally requires claims within 12 months of the date of service, while commercial payer deadlines often range from 90–180 days. Always verify requirements with each payer.
Q4: Are different CPT codes used for group and individual psychotherapy?
Yes. Individual psychotherapy uses CPT codes 90832, 90834, or 90837 based on session length. Group psychotherapy is reported with CPT 90853 and is billed per patient per session.
Q5: How do you bill mental health services for patients with both Medicare and Medicaid?
For dual-eligible patients, Medicare is typically billed as the primary payer, and Medicaid may cover remaining cost-sharing amounts based on coordination-of-benefits rules. Follow payer-specific submission requirements.
Conclusion
Mental health billing in 2026 requires more than accurate CPT coding. Practices need reliable systems for documentation, authorization tracking, telehealth compliance, and denial prevention to protect reimbursement.
Whether managed in-house or supported by a specialized billing partner, a proactive revenue cycle approach can help behavioral health practices reduce claim issues and improve financial performance.
If your practice is experiencing rising denials, authorization challenges, or billing workflow gaps, consider a behavioral health billing assessment to identify opportunities for improvement.
